Machine learning classification for pricing medical services
The data I selected comes from:https://meps.ahrq.gov/mepsweb/data_stats/Pub_ProdResults_Details.jsp?pt=Statistical%20Brief&opt=2&id=1308 This study analyzed the impact of medical services on pricing. I first clarified my research goal to provide clearer pricing logic for healthcare service providers. So I chose decision tree and neural network regression.
Because healthcare providers have a significant differentiation in service types and operations, I hope to use these contents as inputs to maximize the inclusiveness of the model. I used a standardizer and saved the model parameters In order to automate the entire process using scaler in the subsequent pricing analysis.
Methodology:
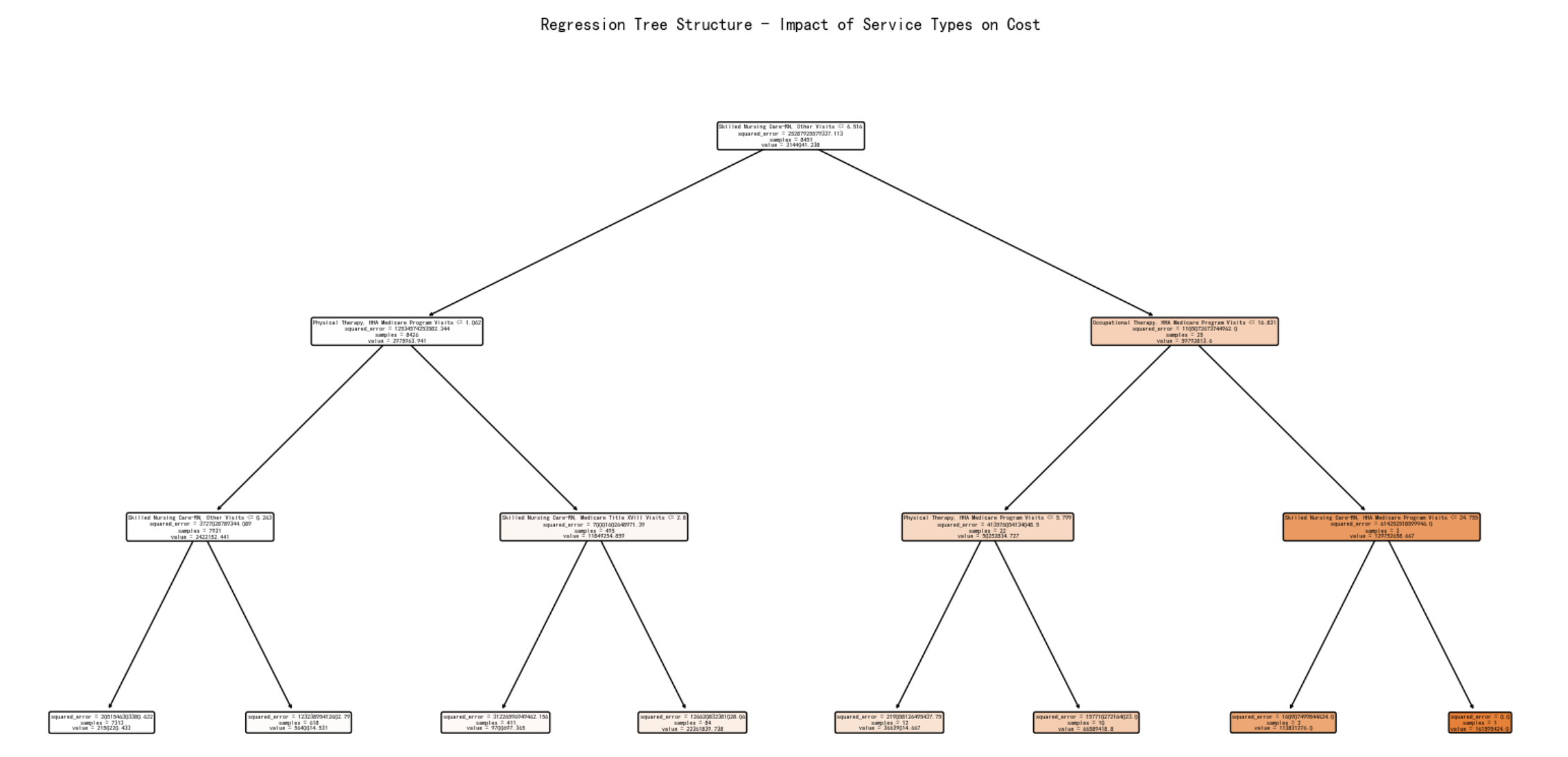
Decision Tree was employed to identify critical thresholds of service quality indicators (e.g., specialist availability, equipment level), creating rule-based segmentation of healthcare institutions.
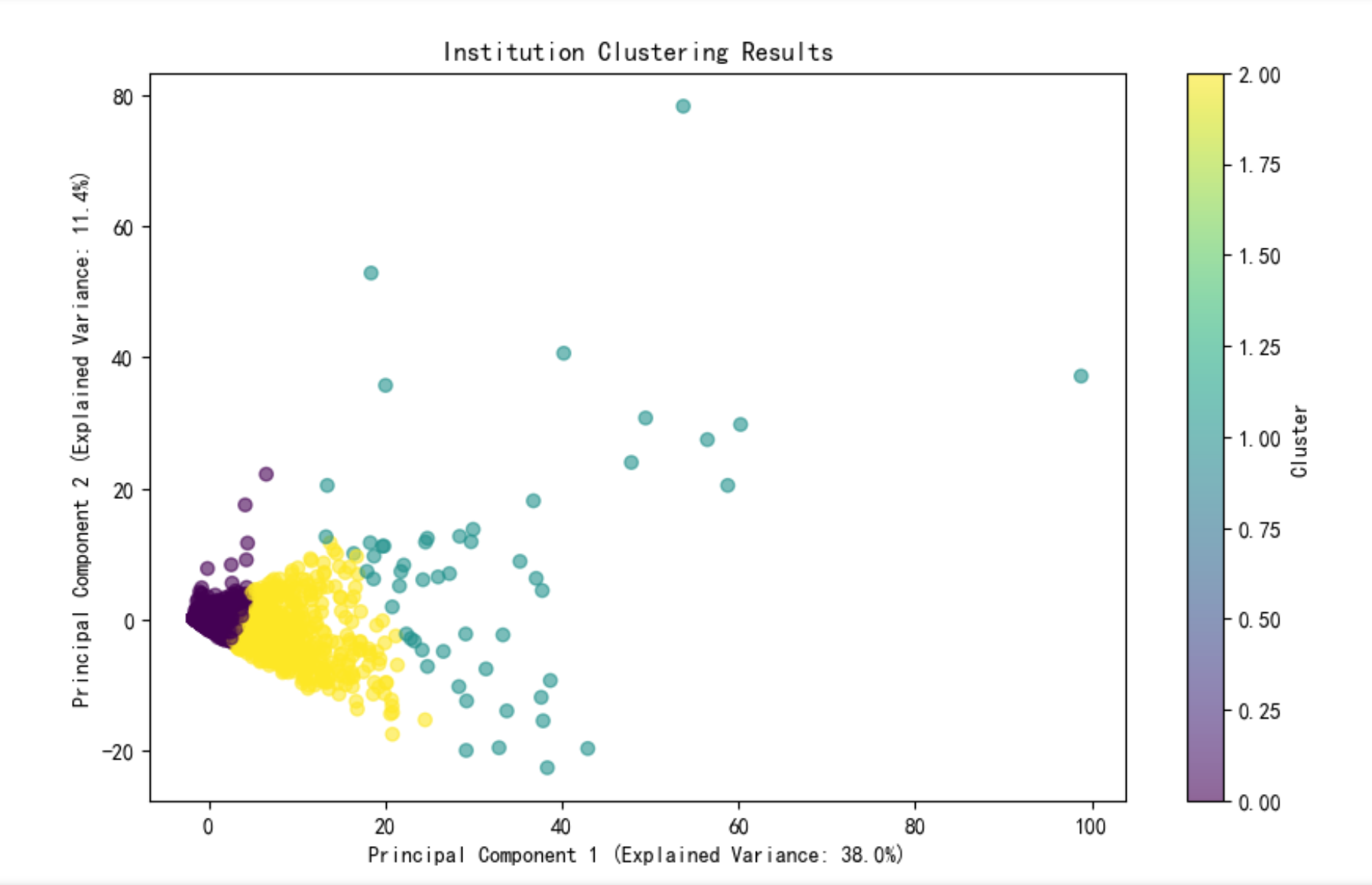
K-means Clustering categorized providers into three distinct groups based on operational efficiency metrics derived from service capacity and cost structures.
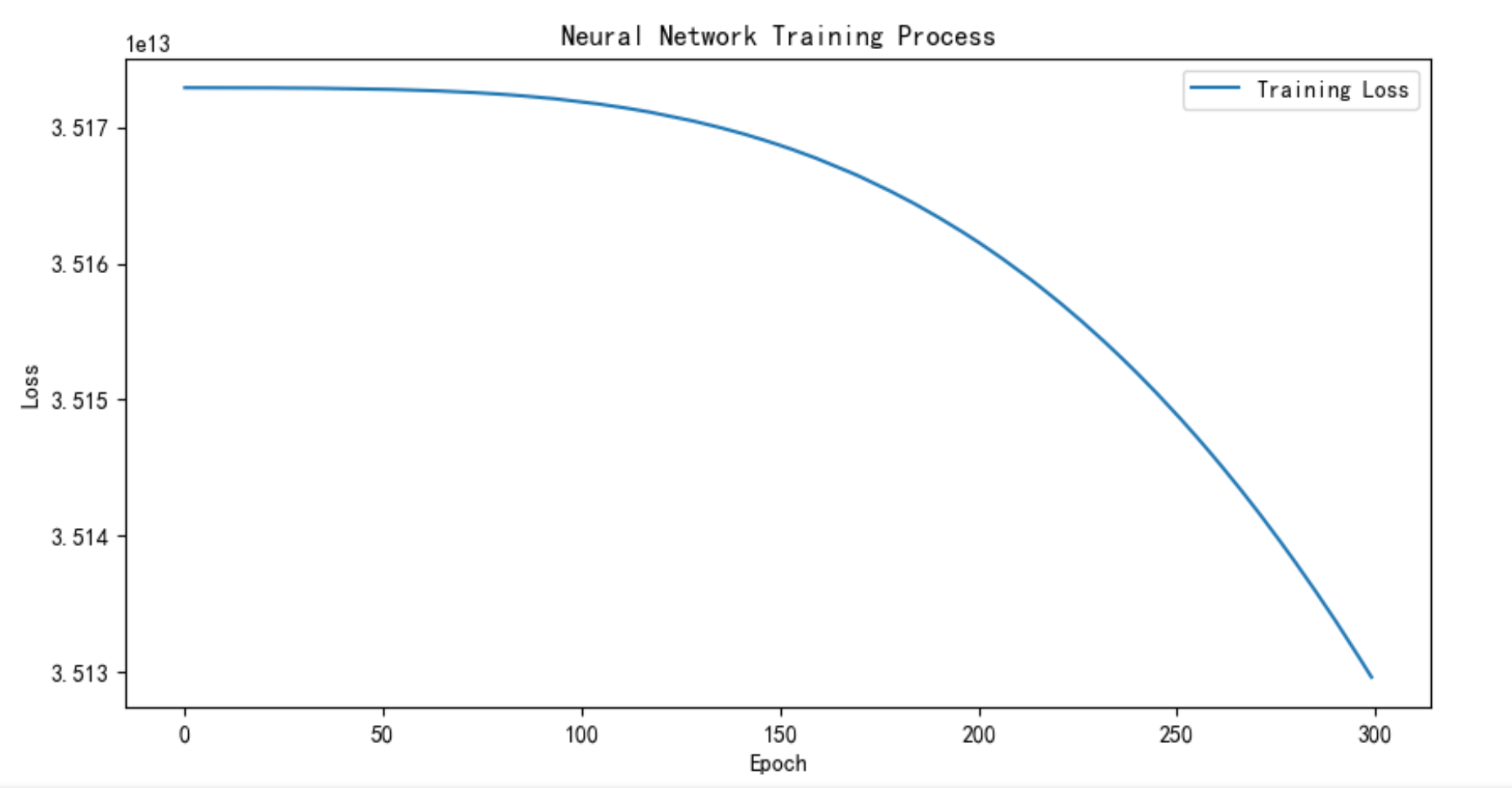
Neural Network Regression (MLP-based) predicted optimal pricing ranges by learning non-linear relationships between service features, operational clusters, and historical pricing patterns.
Technical Implementation:
A standardized pipeline integrating MinMaxScaler for feature normalization and model components was containerized for deployment.
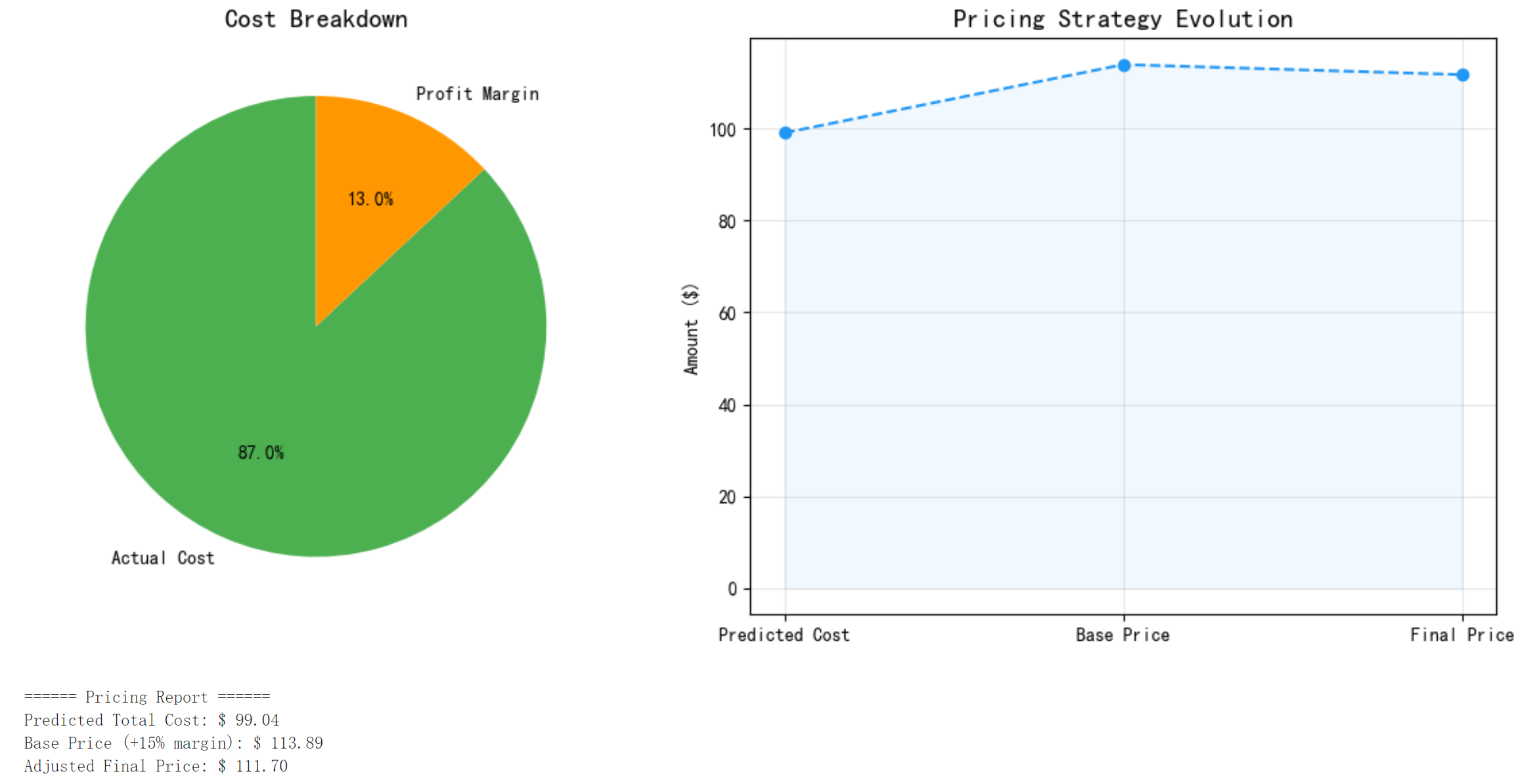
The modular system allows providers to input weighted features corresponding to their strategic priorities (e.g., premium services vs cost efficiency), generating customized price suggestions through dynamic model orchestration.
Prcing
This framework demonstrates how interpretable machine learning techniques can bridge operational analytics with market-responsive pricing strategies in healthcare services.
Markdown:
The data from CDC is enormous, containing hundreds of features. There are countless research paths, we can adopt different model combinations according to different purposes, such as:
-
- Cost driven factor analysis (interpretability model)
- What the model does: Identify which input features (such as complications, medication plans, etc.) contribute the most to predicting costs.
- Principle: On existing regression or classification models, apply algorithms such as SHAP/LIME to quantify the positive and negative impact of each feature on the “model output” (cost).
-
- High cost patient identification (classification model)
- What does the model do: Classify patients into “high cost” vs “non high cost” categories to facilitate pre screening of potential heavy spending populations.
- Principle: Using logistic regression, decision trees, deep classifiers, etc., treat cost labels (such as>a certain threshold) as categories and learn the mapping of “features → categories”.
-
- Analysis of Cost Sub item Structure (Multiple Output Regression or Branch Model)
- What does the model do: simultaneously predict the proportion or absolute value of multiple sub item costs such as medication fees, examination fees, and surgical fees.
- Principle: Use a multi output regression network or branch out multiple “sub networks” at the last layer to predict different cost types.
-
- Spending time series pattern mining (sequence model)
- What does the model do: Based on the cost time series of the patient’s past multiple visits, predict the cost fluctuations for the next or future cycle.
- Principle: Use time series models such as RNN/LSTM/Transformer to capture the “sequence” and “autocorrelation” for dynamic prediction.
-
- Cost based Clustering
- What does the model do: Automatically classify patients into several categories based on “cost+characteristics” (such as low, medium, and high cost groups) for differentiated management.
- Principle: Use unsupervised learning methods such as K-means, hierarchical clustering, or spectral clustering to cluster samples into the same cluster based on distance or similarity.
-
- Pricing and Optimization of Insurance Products (Simulation and Optimization Models)
- What does the model do: Simulate the cost sharing results between patients and insurance companies under different deductibles, reimbursement ratios, and other parameters, and find the optimal combination.
- Principle: First, estimate the cost distribution using a regression model, and then run Monte Carlo simulation or solve linear/nonlinear optimization problems based on this.